目前对无症状肾积水的评估和处理仍然存在争议。有学者提出大部分胎儿肾积水可在妊娠晚期或新生儿期自愈[4]。然而,Chertin等[2]报道超过50%的肾积水患儿因肾功能恶化而行手术治疗。积水的进展和肾功能的恶化作为目前手术治疗的指征,但胎儿肾积水的哪些患儿可自愈,哪些需在肾功能恶化前行手术治疗,乃存在争议。
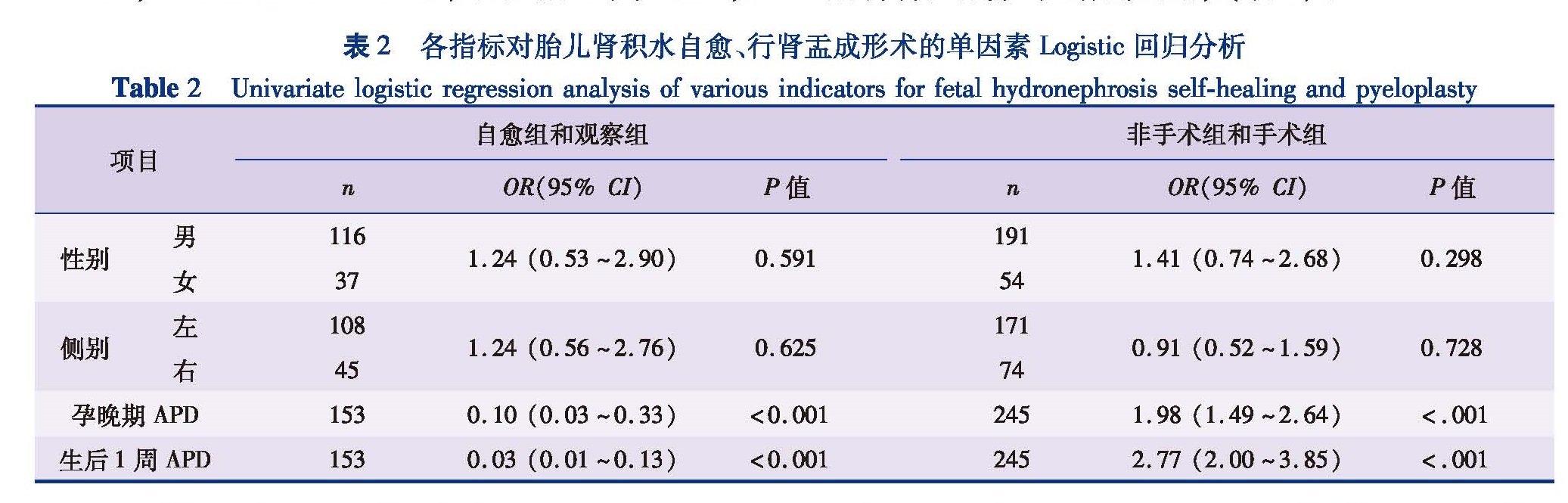
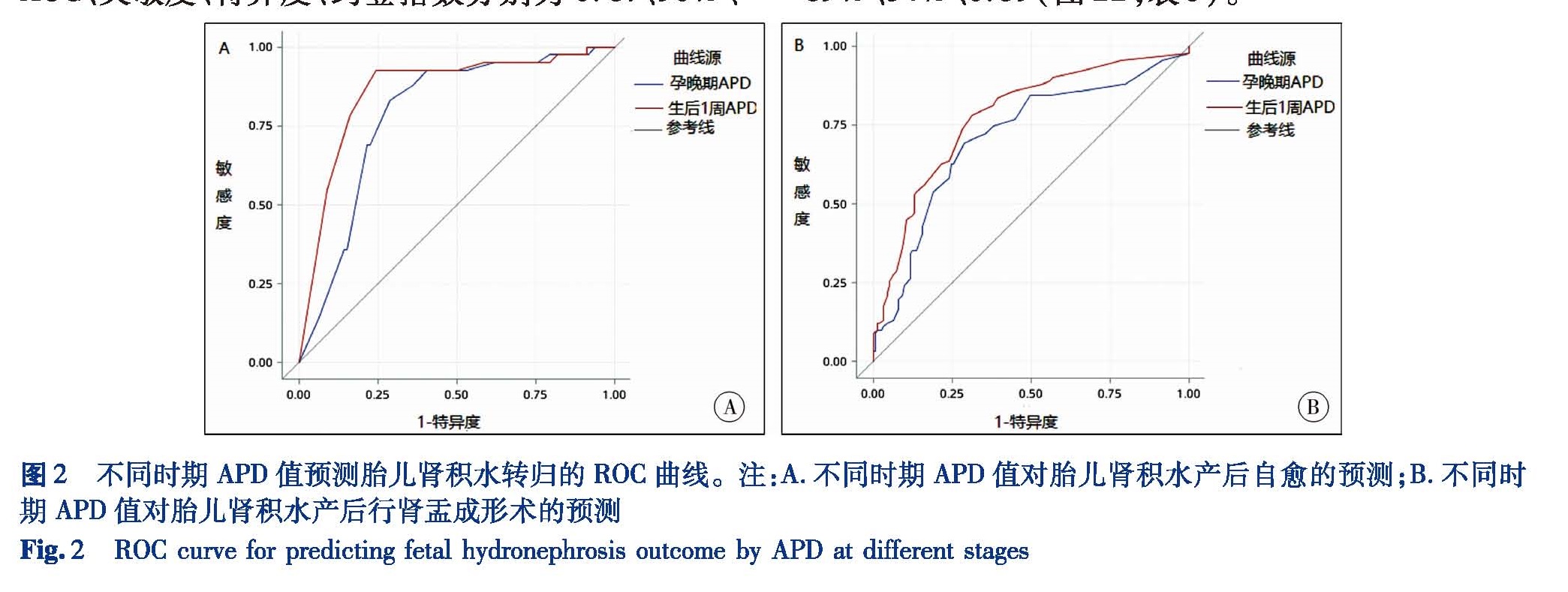
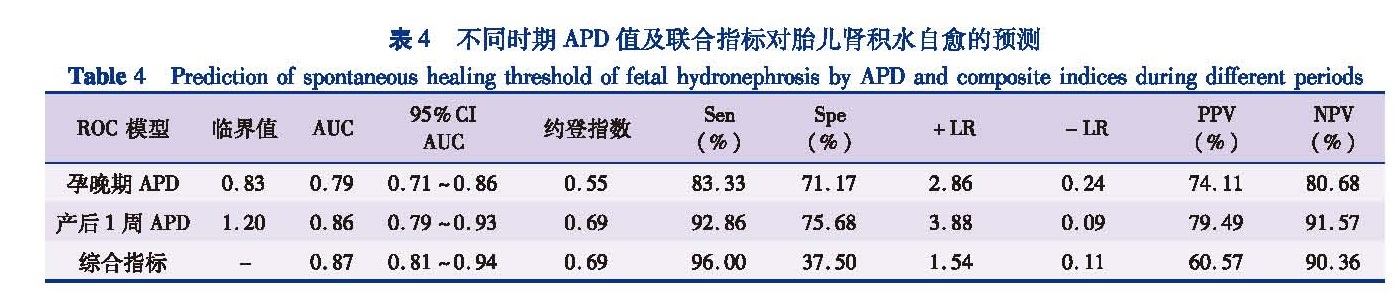
妊娠晚期及新生儿期自愈是胎儿肾积水的特征。由于各中心病例选择不一,报道的胎儿肾积水自愈比例存在较大差异。Alconcher等[5]认为,80%的产前肾积水属于生理性肾积水,无需手术治疗,可以自愈。也有学者认为,自愈期限在13.4~17个月[6],而本研究发现自愈组患儿平均自愈期限为11.4个月,与Alconcher等[5]的研究一致。同时,对预测胎儿肾积水产后是否自愈的孕晚期APD预测值为8.3 mm,敏感性为83%,特异性为71%; 生后1周APD预测值为12 mm,敏感性为93%,特异性为76%,该结果与Anderson[7]的研究一致。此外,由本研究亦可知,孕晚期APD值和生后1周APD值的联合对预测患儿产后自愈的灵敏度较高(96%),优于单一指标。
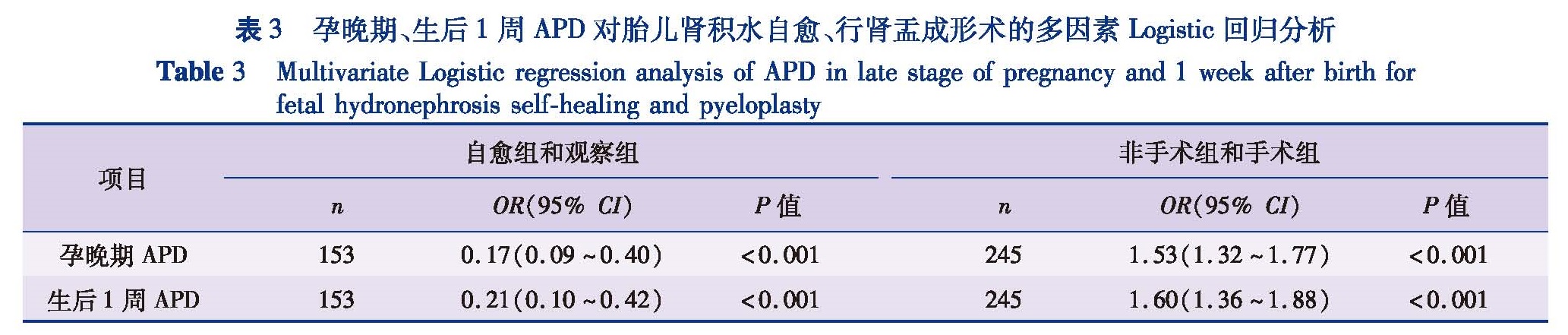
诸多学者认为产前、产后APD值为预测肾盂成形术的重要指标。虽然APD值越高,产后梗阻存在的风险越高,但是目前关于积水患儿肾盂成形术的APD阈值国内外尚无明确定论。本研究发现孕晚期和生后1周APD值为预测肾盂成形术的指标,当孕晚期APD预测值临界点为19 mm时,产后需要行肾盂成形术的敏感性为68%,特异性为71%; 当生后1周APD值的临界点为19 mm时,其预测产后肾盂成形术的敏感性为78%,特异性为69%。Cristina Plevani等[8]对120例(161只肾脏)胎儿肾积水随访研究发现:产前APD(妊娠晚期)值与手术具有相关性(P<0.05)。Mudrik-Zohar等[9]研究发现产前APD值>14 mm预测患儿产后需行肾盂成形术的敏感度为77%,特异度为69%。Longpre等[10]对100例胎儿肾积水(产后病因为UPJO)的临床资料进行分析,得出产后初次超声中APD值为预测产后是否行肾盂成形术唯一的独立危险因素,手术的风险比率为1.4。Arora 等[11]对109只由UPJO所致积水肾脏的随访发现产后初次(产后1周)APD值预测肾盂成形术的敏感度和特异度如下:APD值为15 mm(88.5%和54.2%); APD值为20 mm(88.5%和73.5%); APD值为24 mm(73.1%和88%); APD值为30 mm(26.9%和96.4%),并将产后初次APD值为24 mm作为肾盂成形术的临界值。由于研究样本出于不同的临床中心,加之样本量的不同及超声检查的主观性,造成肾盂成形术的预测值不同。单纯采用APD值预测胎儿肾积水预后简便易行,但实际工作中,衡量患儿手术的指标还包括肾实质厚度、DRF、积水是否进展、分肾功能下降程度等,因而临床医生应全面仔细考虑。
有学者提出通过联合产前、产后APD值以提高预测胎儿肾积水行肾盂成形术的准确性。巴西一项研究发现:胎儿期APD值>18 mm且患儿生后APD值>16 mm,需要产后手术治疗的敏感度为100%,特异度86%[12]。本研究发现孕晚期APD值≥19 mm或生后1周APD值≥19 mm对预测患儿产后行肾盂成形术的灵敏度较高(89%),优于单一指标。
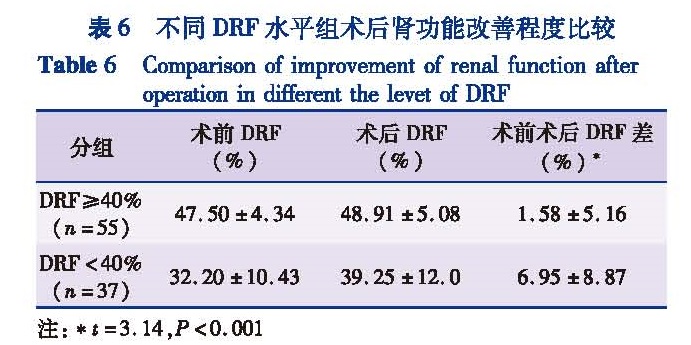
对于肾盂成形术后患侧肾功能能否改善,目前仍存在争议。多位学者的随访研究发现肾盂成形术后患儿的DRF能得到改善,并将术前DRF<40%作为手术指征。Rosen[13]等研究发现肾实质非常菲薄的积水肾,其小管间质仍然可能仅受轻微的损伤。进而表明手术解除梗阻后,患肾的分肾功能有能够得到很好恢复的客观基础。但术前分肾功能低的患肾在术后分肾功能有更大的恢复空间,而对于术前分肾功能正常或略低的患肾在术后则没有进一步提高的空间[14]。Harraz[14]等对196例2个月~18岁行肾盂成形术患儿进行长期随访发现96例术后患肾功能改善超过5%,并认为术前DRF<40%的患者术后患肾功能得到改善。而Calisti[15]等认为产前诊断的肾积水多为内源性梗阻,并且常常合并先天性肾脏损害,因此术后肾脏功能改善不明显。McAleer等[16]对79例行肾盂成形术的患儿进行随访发现术前、术后DRF改变均无统计学意义(P=0.078){出现肾瘢痕患儿(P=0.38),DRF≤40%患儿(P=0.46),DRF≥40%患儿(P=0.065)}。本研究中,29例患儿行肾盂成形术后DRF增加超过5%,其中术前DRF≥40%组有11例患儿,DRF<40%组有18例患儿,这说明术后患肾DRF能得到改善,且术前DRF<40%组术后DRF改善程度明显高于术前DRF≥40%组术后DRF的改善程度,这与Harraz等[14]的研究结果一致。此外,本研究还发现手术患儿中术前DRF<40%组术后患肾功能的恢复仍未达到术前DRF≥40%组的术后患肾功能。
本研究表明,19.1%的Ⅱ度肾积水患者最终行手术治疗。因此,产前检出的全部I度和大多数Ⅱ度肾积水患儿预后良好,不需要手术干预。对于SFUⅢ度肾积水患儿,约41.8%术前DRF≥40%,16.3%术前DRF<40%Ⅲ度肾积水患儿最终行手术治疗,因此,对于SFUⅢ度肾积水患儿应该密切监测积水程度及肾功能,存在梗阻征象时进行手术治疗。对于SFUIV度肾积水,43.1%术前DRF≥40%,43.6%术前DRF<40%Ⅳ度肾积水患儿最终行手术治疗。因此,我们建议对于这类患儿在密切的临床监测后及时进行手术治疗对保护患肾功能有利。
综上所述,产前超声和产后随访是评价胎儿肾积水预后的有效方法。利用超声检查指标,了解积水的程度,预测其预后及转归,有助于临床医生采取及时有效的监测及干预措施,预防肾脏功能的恶化。小儿肾积水手术解除梗阻后,患肾功能是可以得到改善的,因而对于明确为病理性肾积水的患儿需早期手术干预解除病因以保护肾功能。
![表1 性别、侧别的分布[n(%)]<br/>Table 1 Distributions of gender and sideness[n(%)]](2018年06期/pic01.jpg)