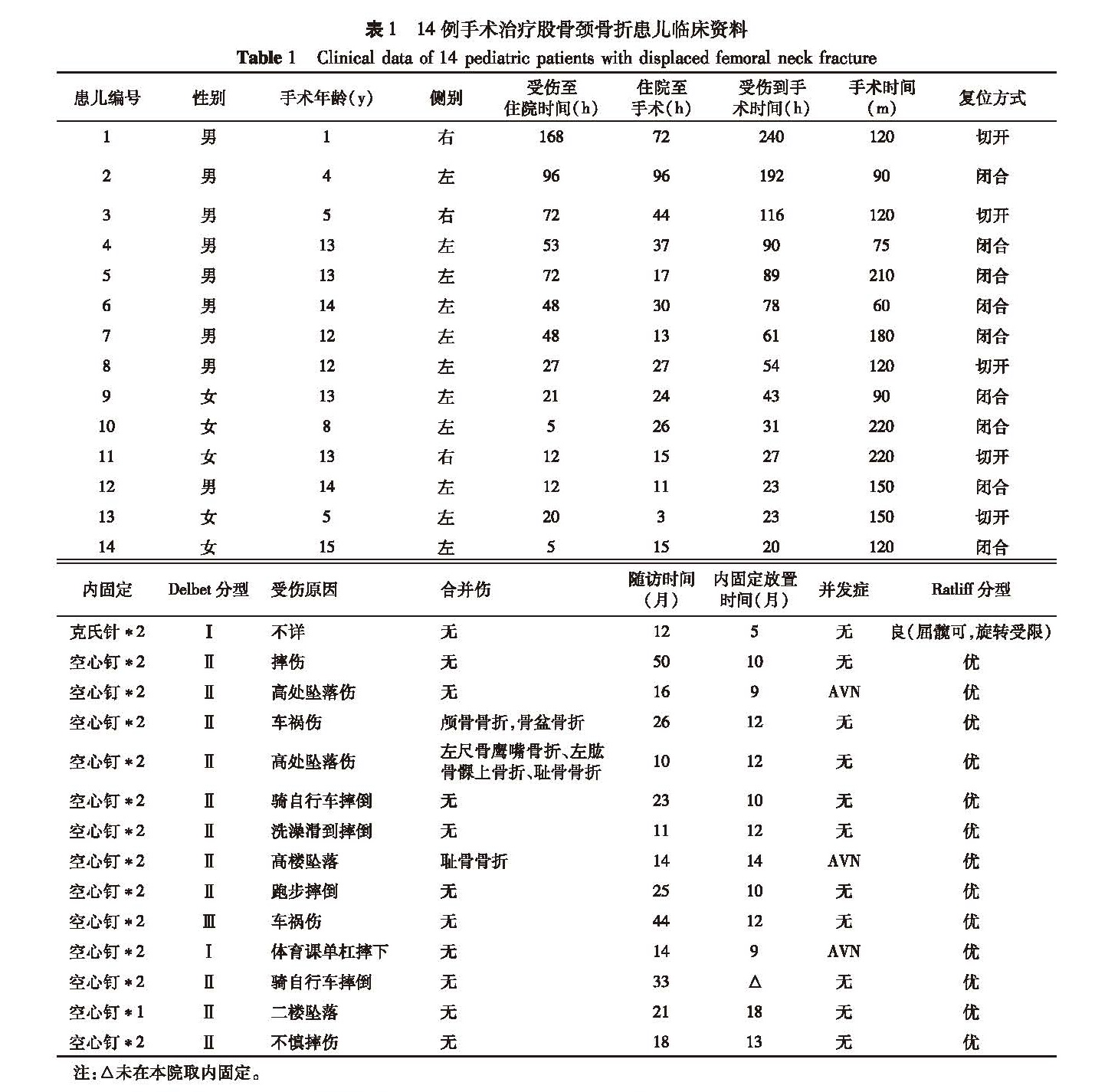
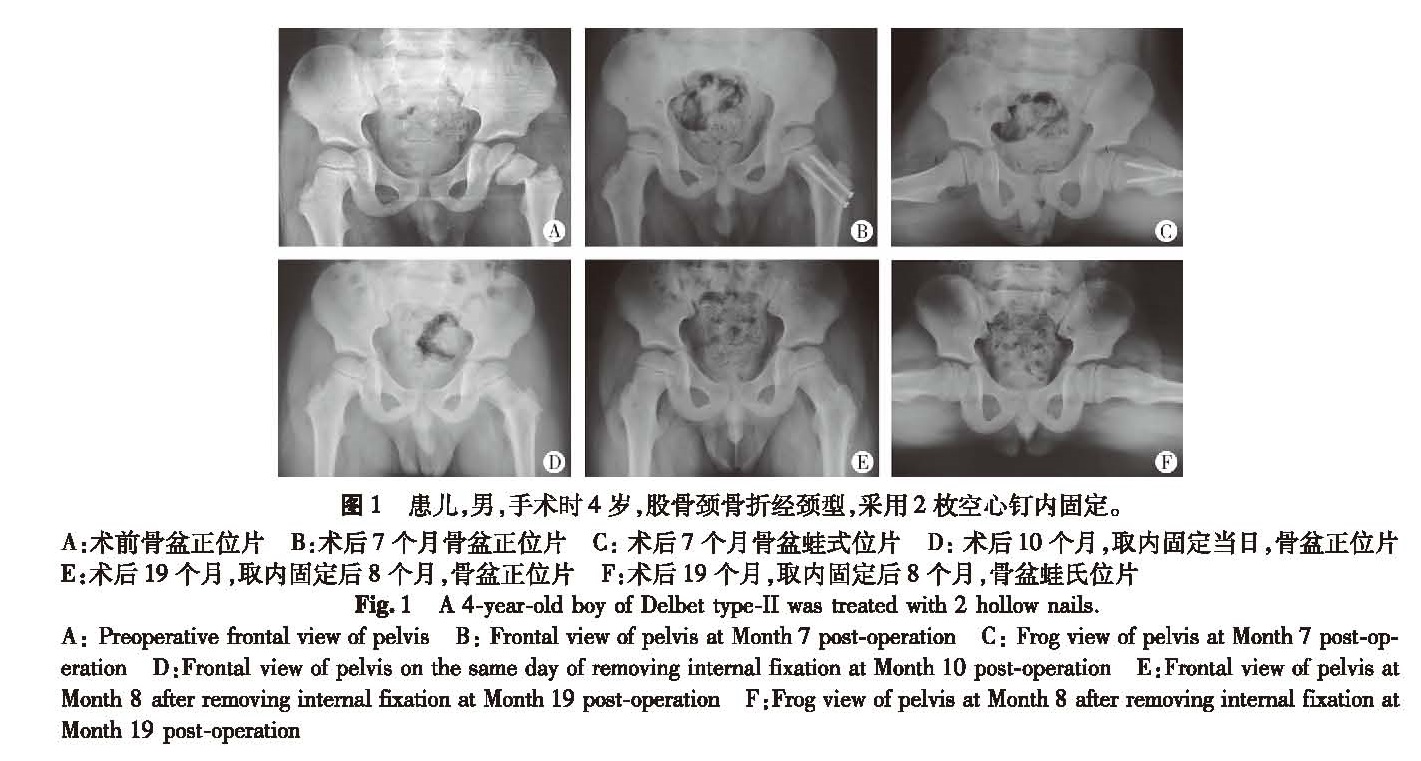
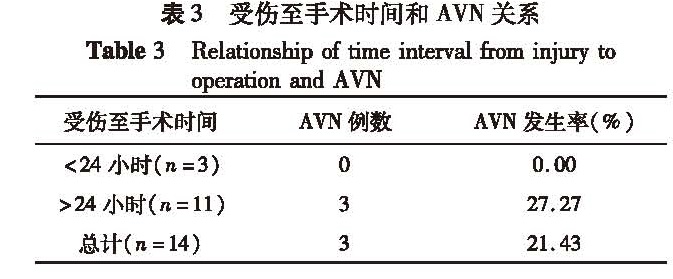
目的 回顾性分析14例不同类型移位股骨颈骨折患儿的临床资料,分析手术复位内固定治疗后的并发症及疗效。 方法 对2010年9月至2014年6月间经本院手术治疗的14例移位股骨颈骨折患儿进行回顾性分析。其中男9例,女5例; 右髋3例,左髋11例; 头下型2例,经颈型11例,基底型1例; 平均年龄10.1岁。急诊手术首选闭合复位,髋关节囊予以抽吸淤血减压; 如不成功,予以切开复位,同时清除关节囊内积血等减压。复位后常规予空心钉或克氏针内固定,再予髋人字石膏固定至少2个月。采用Ratliff评分评估功能恢复情况。 结果 14例患儿中高处坠落伤4例,车祸2例,跑步、骑自行车摔倒等外伤7例,无明显外伤史1例。受伤至手术时间间隔平均77.6 h(20~240 h)。手术时间平均136 min(60~220 min)。闭合复位+关节囊抽取积血减压9例,切开复位5例。内固定时间平均为11.2个月。术后患儿随访时间平均为22.6个月(10~50个月)。术后股骨头缺血性坏死(AVN)发生率头下型1例(50%),经颈型2例(18%),基底型无一例。出现AVN的3例患儿受伤至手术时间均大于24 h。 结论 小儿单纯摔倒和骑车摔倒甚至无明显重大外伤史情况下也可出现股骨颈骨折。由于儿童股骨头血供特点和儿童自身发育,越接近股骨头处骨折因血供不足越易出现股骨头缺血性坏死,头下型和经颈型分别占前二位。伤后需急诊早期手术复位骨折内固定,关节囊减压,术后坚强外固定,这三者都有利于防止股骨颈骨折并发症的发生。
Objective To explore the influencing factors of displaced femoral neck fracture(DFNF)in children. Methods A retrospective review was conducted for 14 DFNF children between September 2010 and June 2014. There were 9 boys and 5 girls with an average age of 10.1 years. The involved hips were right(n=3)and left(n=11). There were Delbet type-Ⅰ(n=2), Delbet type-Ⅱ(n=11)and Delbet type-Ⅲ(n=1). They were divided into two groups of closed reduction & internal fixation(CRIF,n=9)and open reduction & internal fixation(ORIF,n=5). Casting was applied for at least 2 months. Complications were observed and short-term effectiveness was evaluated by Ratliff standard. Results The causes were falling from height(n=4), traffic accidents(n=2), falling to the ground during running or biking(n=7)and no obvious sigh of trauma(n=1). The average interval from injury to surgery was 76(20-240)hours and average operative duration 136(60-220)min. Internal fixation was removed at an average of 11.2 months post-operation. The average follow-up period was 22.6(10-50)months. Avascular necrosis(AVN)occurred in Delbet type-Ⅰ(n=1,50%)and Delbet type-Ⅱ(n=2,18%).The occurring interval from injury to surgery was over 24 hours. Conclusion DFNF results from falling to the ground or off bicycle even without a significant trauma history. Because of hemodynamic and growth characteristics of femoral head in children, fractures closer to femoral head, AVN is more likely to occur, especially Delbet type-Ⅰ and type-Ⅱ. Reduction early and internal fixation, joint capsule decompression and adequate postoperative external fixation are conducive for preventing the occurrence of DFNF complications.