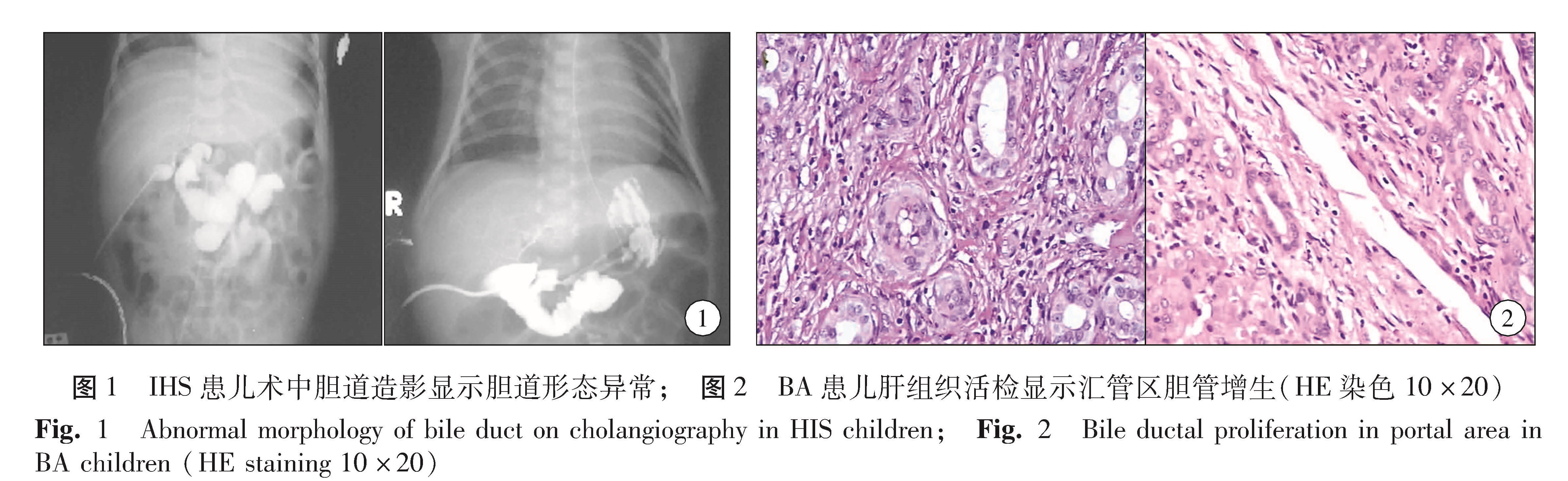
新生儿及婴幼儿黄疸病因较复杂,鉴别诊断困难,是临床诊断治疗的难点,主要包括BA及IHS两种。BA是新生儿及婴幼儿阻塞性黄疸的主要病因,发病率约为1/8 000~1/14 000。根据患儿临床表现不同可分为围产期型及胚胎型,围产期型占80%,这些患儿出生时胆道存在,在新生儿期病原侵袭、炎症进展而出现胆道纤维闭锁。其特征为较迟出现黄疸,在生理性黄疸消退后再次出现黄疸。胚胎型占20%,其特征为生后持续性黄疸。IHS是以黄疸、肝脏及胆道系统病损、肝脏增大,肝功能异常为特征的临床征候群,通常由感染及代谢性疾病所致。两者在临床表现上往往难以区分,需尽早手术探查,术中行胆道造影以明确胆道通畅情况。近年诸多研究表明,病毒感染是BA及IHS的主要病因,病毒感染可发展为胆道闭锁[1-5],病毒感染亦可用于判断胆道闭锁预后[12]。在临床工作中,对近40例内科疗效不佳的黄疸患儿进行腹腔镜胆道探查,术中于胆囊插管行胆道造影。其中7例胆道存在,故行胆囊造瘘术,术后诊断为IHS; 约30余例诊断为BA,除外放弃治疗者共行Kasai术25例。在确诊为IHS的患儿胆道造影平片中,5例形态异常,表现为肝内外胆管细线样或胆管腔毛糙不光滑。结合IHS与BA病因相似,是否这部分患儿最终发展为BA,为BA的前期表现,尚未见文献报道,值得我们探讨。本文就内科疗效不佳的黄疸患儿,术中造影表现为胆道异常者与BA患儿肝组织活检病理表现作对比,推测胆道造影异常的IHS与BA是否存在疾病相关性。
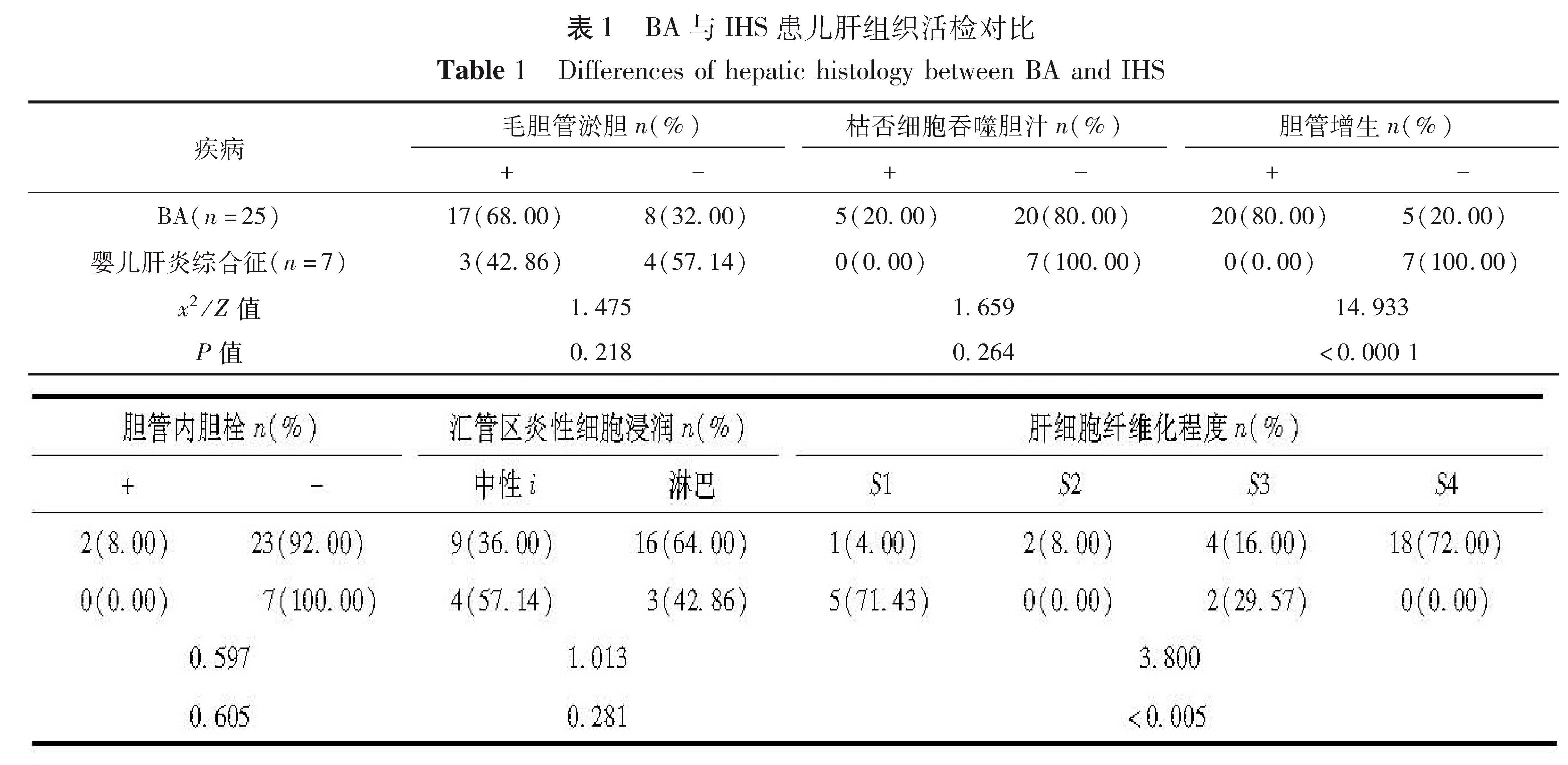
肝组织活检是鉴别胆道闭锁及其它胆汁淤积性肝病的重要方法,其准确性可以达到88.2%~96.8%,在欧美等发达国家及发展中国家被作为胆道闭锁的主要诊断方式之一[6], 内容包括实质细胞改变(包括肝细胞羽毛变性、毛胆管扩张淤胆、枯否细胞吞噬胆汁),是梗阻及非梗阻性黄疸患者共同存在的非特异性表现; 而汇管区胆管增生、胆栓形成、水肿及中性粒细胞浸润为BA特有的病理表现。应用肝活检评分系统有助于诊断胆道闭锁,敏感度达94.7%,特异度达86.2%,准确率达91.9%[9]。本研究对IHS及BA患儿手术肝组织活检病理表现作了详细比较,发现BA患儿与IHS患儿在肝细胞淤胆、毛胆管淤胆、枯否细胞吞噬胆汁三种非特异性淤胆上的表现无明显差异,提示两者均存在肝细胞胆汁排泄障碍及胆管胆汁淤滞现象。但汇管区胆管增生数目在BA中明显增多,统计分析两者存在明显差异(P<0.0 001)。与Li等报道一致[7,10,13],故认为汇管区胆管增生是BA肝组织活检各项指标中最具诊断价值的指标。但胆栓形成、水肿及中性粒细胞浸润三种病理表现在本研究中BA患儿与IHS患儿未见明显差异(P>0.05),与部分现有报道不符,需进一步研究验证。
同时,本研究发现,BA患儿肝纤维化程度明显高于IHS患儿(P<0.005),考虑与胆道梗阻后肝脏损害进一步加重,病情进展快,肝细胞死亡及纤维再生迅速,导致快速形成肝纤维化有关。因此,该研究结果不支持IHS是BA前期病变的假设。
在IHS患儿中,5例胆道造影呈细线样胆道,合并胆管壁毛糙,经短期随访,除1例因肝细胞坏死严重(病理检查提示大部分肝细胞变性坏死)、肝功能差而于术后出现肝功能衰竭死亡外,其余4例均黄疸消退、大便转黄、临床症状完全缓解而治愈。提示胆道细线样形态异常可经胆道冲洗及保肝治疗痊愈,而不会进展为BA。
综上所述,本研究结论如下: ①虽然IHS与BA有相似的病因,且胆道造影在IHS患儿存在胆道形态异常,但两者肝组织活检病理表现存在明显差异。IHS患儿肝组织活检不具备梗阻性黄疸的病理特征,且随访发现患儿均可通过保守治疗而治愈,故不提示IHS合并胆道形态异常患儿是BA的前期表现,两者可能具有不同发病过程。进一步研究可通过大样本胆道形态异常IHS患儿术后保留胆囊造瘘管,择期行胆道造影而明确其形态的动态变化。②肝穿刺活检病理显示汇管区小胆管增生及肝纤维化程度较高(>S3级),对提示BA具有一定的指导意义,可作为临床诊断BA的辅助检查之一。