相对于成人鞘膜积液病因的不同,持续开放的鞘状突管(PPV)是儿童鞘膜积液的共同病因,约有60%的婴儿会出现,而在成人则可能是鞘膜囊内分泌的原因[3-4]。所以,儿童鞘膜积液的手术方法也与成人不同,关闭开放的PPV即可起到良好的效果。囊肿内积液可穿刺排出或打开放液,亦可不做处理。不必行鞘膜翻转或鞘膜切除术[5]。作为鞘状突不断变化的结果,Naji H[6]等报道在年龄1岁以下的婴儿中约有89%的PPV会自然闭合。目前,尚没有文献说明儿童鞘膜积液需要手术的确切时间。通常,如果儿童鞘膜积液持续存在超过12~24个月,则需要外科干预[1]。但如果张力较高,可能影响睾丸血液循环,手术治疗不受年龄限制[4]。
采用腹腔镜手术治疗鞘膜积液主要归功于腹腔镜手术修补儿童腹股沟疝的成熟与推广。腹腔镜手术治疗鞘状突未闭的外科原则是解剖上闭合持续开放的PPV[7],这与儿童腹股沟疝的治疗是一致的,其可行性与安全性已在各中心的一些研究中证实[8-10]。虽然以往有人认为仅交通性鞘膜积液才可以采用腹腔镜手术方式,但在我们的研究中腹腔镜下99.6%的患儿在内环口处可发现开放的PPV,进行单纯的PPV环扎治疗后取得了理想的效果。仅4例(0.4%)患儿经腹腔镜探查确实未发现开放的PPV内口,而改为经阴囊的睾丸鞘膜翻转手术,整个操作过程的创伤明显低于传统经腹股沟探查手术。我们认为鞘膜积液与腹股沟斜疝相比,其PPV内口小且光滑,输精管清楚,没有增厚的腹膜和瘢痕组织,更加适合腹腔镜手术。
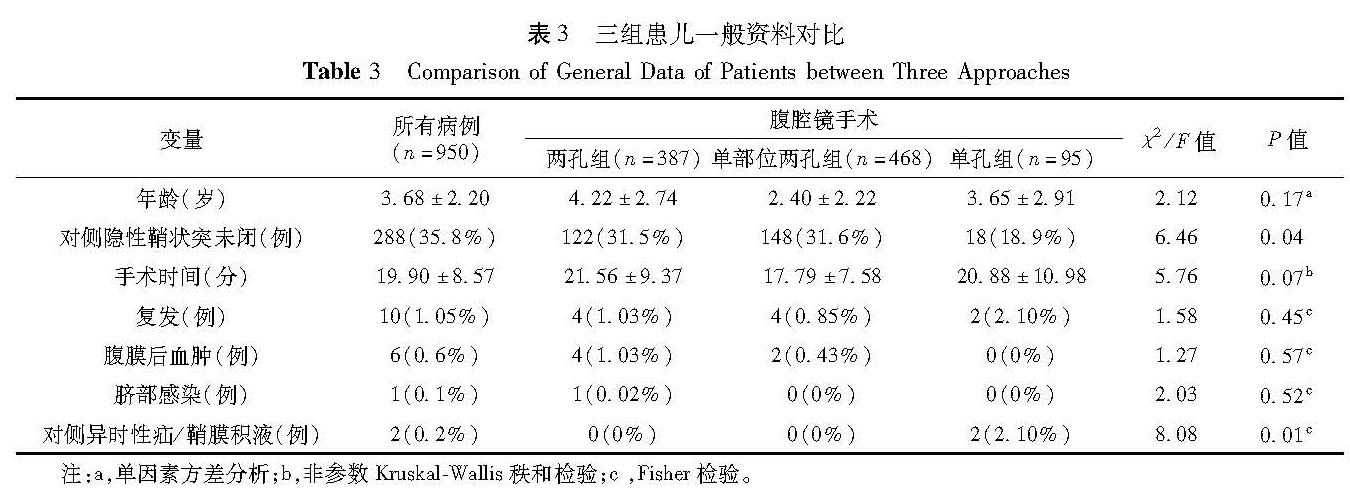
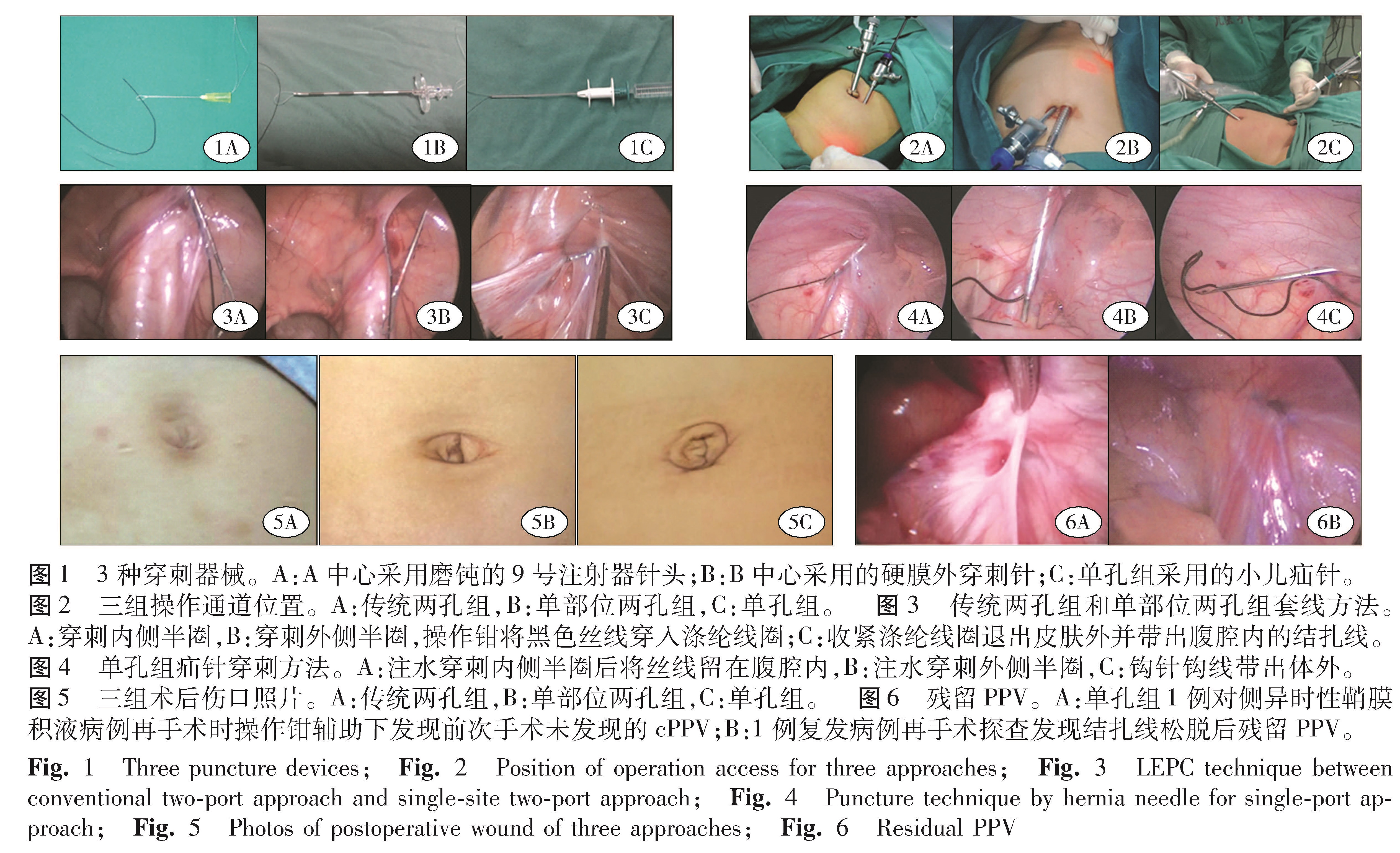
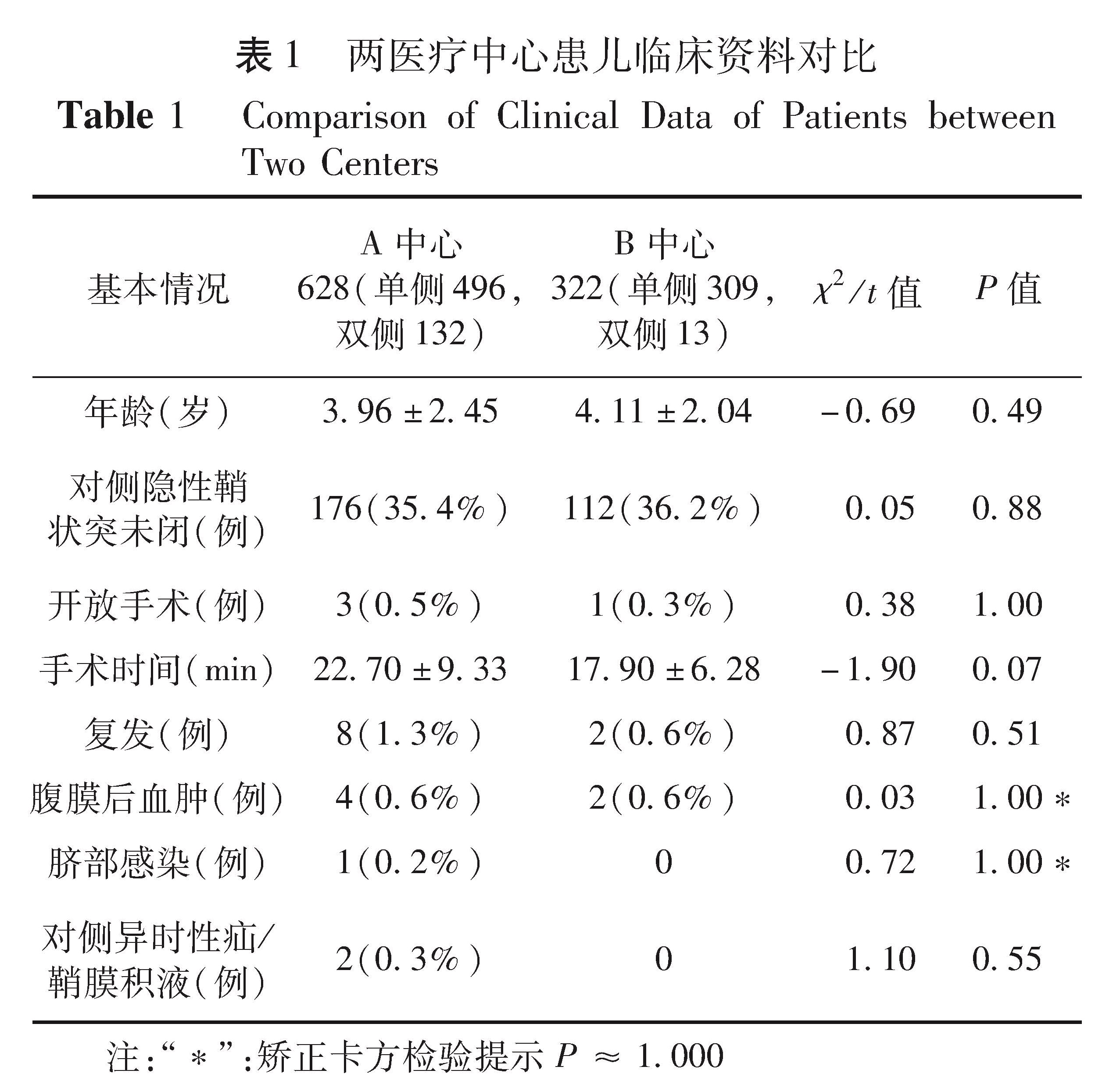
Takehara H[11]等自1995年开始采用腹腔镜下经皮腹膜外内环结扎术(laparoscopic percutaneous extraperitoneal closure,LPEC)治疗儿童腹股沟疝并取得了成功。此后许多的LPEC改进技术被不断报道,其不同之处在于使用各种LPEC操作设备,如自制疝针、Endoclose针、GraNee针、Reverdin骨穿缝合针、皮下注射针、普通缝合针、硬膜外针等作为缝合器具,或者采用一体式目镜和操作钳设备[12-14]。我们在经过多种方法尝试后总结经验认为采用可注水的小儿疝钩针的优点在于使用单孔操作通道即可完成手术,而采用磨钝的9号注射器针头和硬膜外针的方法完成两孔法LEPC手术也具有以下优点: ①相比各种专门的一次性疝针,我们的材料简便易得、性价比高,可以应用于大量日间手术; ②穿刺口小,较各种疝针更加美观; ③握针轻巧灵活,方便分离,同样可以进行注水等操作。有学者认为腹膜后血肿与穿刺针过于锐利有关,而本研究使用的针(尖)头相对不锐利,故认为造成血肿的原因主要和手术操作熟练程度有关,而与针的粗细无关。本组腹膜后血肿共6例(0.6%),均出现在手术的学习曲线早期。我们认为当使用较细的穿刺针刺破血管时损伤相对较小,出血容易自行停止。而采用注射器针和硬膜外针的不足就是需要另一把操作钳的辅助才能完成手术。但是有一把辅助操作钳的优势也毋庸置疑: ①可以更快、更确切的完成腹膜内缝合,并减少精索、输精管损伤。虽然使用特制疝针通过注水也可以完成缝合,但没有操作钳的辅助,穿刺仍然较困难; ②对cPPV的探查,许多情况下由于有一腹膜褶遮盖了cPPV,往往需要操作钳牵拉显露后方可发现。本研究中单孔组的对侧隐性鞘状突发现率仅18.9%,与两孔组和单部位组比较差异有显著统计学意义(P<0.01),这说明了探查cPPV时操作钳的重要性。国外也有报道采用特殊镜头与操作钳的一体镜,但使用成本高,无法满足大量日间手术病人的需要[14]; ③操作钳牵拉内环口可以检查环扎的可靠性,降低复发率,这是单孔手术无法做到的。
如何降低术后复发率是临床需要面对的主要问题。最常见的复发原因有学习曲线早期、环扎不确切、结扎线松脱和采用了可吸收的结扎线等[15-16]。本组术后复发共10例(1.1%),单孔组复发率达2.1%,且复发并不全部出现在医生学习曲线早期,有部分复发病例出现在有丰富经验的医生中。复发病例中有5例进行了再次手术,术中均可以见到一个PPV缝闭不全留下的残余孔洞,所以我们认为术后复发主要与PPV缝闭不全有关,即使经验丰富的医生也可能有各种原因造成其结扎不确切。对此,我们做了改进: ①缝合和结扎紧贴腹膜进行,减少因为结扎过多皮下组织造成的结扎线松脱; ②对年龄较大的儿童采用较粗的7号丝线结扎,增加线结的确实性; ③结扎完毕后用操作钳检验结扎的可靠性,对有疑虑的病例进行双扎; ④对于单孔手术,我们认为最佳的降低复发率的方法就是进行双扎; ⑤对于单部位双孔道,戳孔要确切选口,保证所插入操作钳的方便灵活使用,避免因两孔口距离太近致镜钳相碰造成操作不便。
对侧隐性鞘状突未闭(cPPV)的处理仍然存在争议[16]。曾有报道cPPV不经处理,其出现疝或鞘膜积液的几率为3%~30%[17]。本研究中单孔组有2例出现术后对侧异时性疝和鞘膜积液,与其他两组比较,差异有显著统计学意义(P<0.01)。所以什么样的cPPV需要处理和怎么样处理能将副损伤降到最低是目前主要争议的问题。因为尚没有确切证据说明哪些cPPV是确实需要外科干预的。我们的经验是对于所有可发现的cPPV都进行处理。对直径大于2 mm的cPPV我们采取环扎治疗,对直径小于2 mm的cPPV我们直接用操作钳将cPPV开口处腹膜牵拉扯破,造成一个环形创面。通过对复发病例再手术时的观察可以发现,这样处理过的腹膜已经愈合成一个整体,cPPV消失。
对于操作通道的不同,目前多数文献报道疝和鞘膜积液的腹腔镜治疗趋于向单孔、单切口腹腔镜技术的发展[1-2,12-13]。但是本研究结果显示环脐单部位两孔方法更为适合腹腔镜治疗儿童鞘膜积液。从手术操作上看,单部位两孔法与传统两孔法在操作难度和疗效上无明显差别; 从手术创伤上看,单部位两孔组在术后6 h的疼痛FLACC评分与单孔组均不超过2分,也没有出现因为多一个套管引起穿刺损伤的不良事件。在伤口外观上,术后1年左右已经基本无法分辨单部位两孔组和单孔组脐部伤口的差别。对于一些单孔双通道的手术方法,即在脐部一个切口内置入目镜通道和一把操作器械进行手术,我们认为其操作难度大于单部位两孔方法,而实际伤口外观较单部位两孔法并没有优势。
综上所述,我们认为LPEC治疗儿童鞘膜积液安全、有效、操作简便,其中环脐单部位两孔方法的疗效与传统两孔法相同,而操作的可行性、安全性较单孔法高,美观效果也不亚于单孔法。本研究不足之处在于成人鞘膜积液为鞘膜囊内分泌的可能大,腹腔镜手术未处理的鞘膜囊是否会在今后再次形成非交通性鞘膜积液,需要长期随访研究证实。
![表2 三组病例病变侧别情况[n(%)]<br/>Table 2 Affected sides of Three Groups[n(%)]](2017年01期/pic31.jpg)